Airway Management
Cricothyrotomy (Emergency Surgical Airway)
Emergency cricothyrotomy (surgical airway) - technique, indications, and management for cannot-intubate-cannot-oxygenate situations.
Emergency cricothyrotomy (surgical airway) - technique, indications, and management for cannot-intubate-cannot-oxygenate situations.
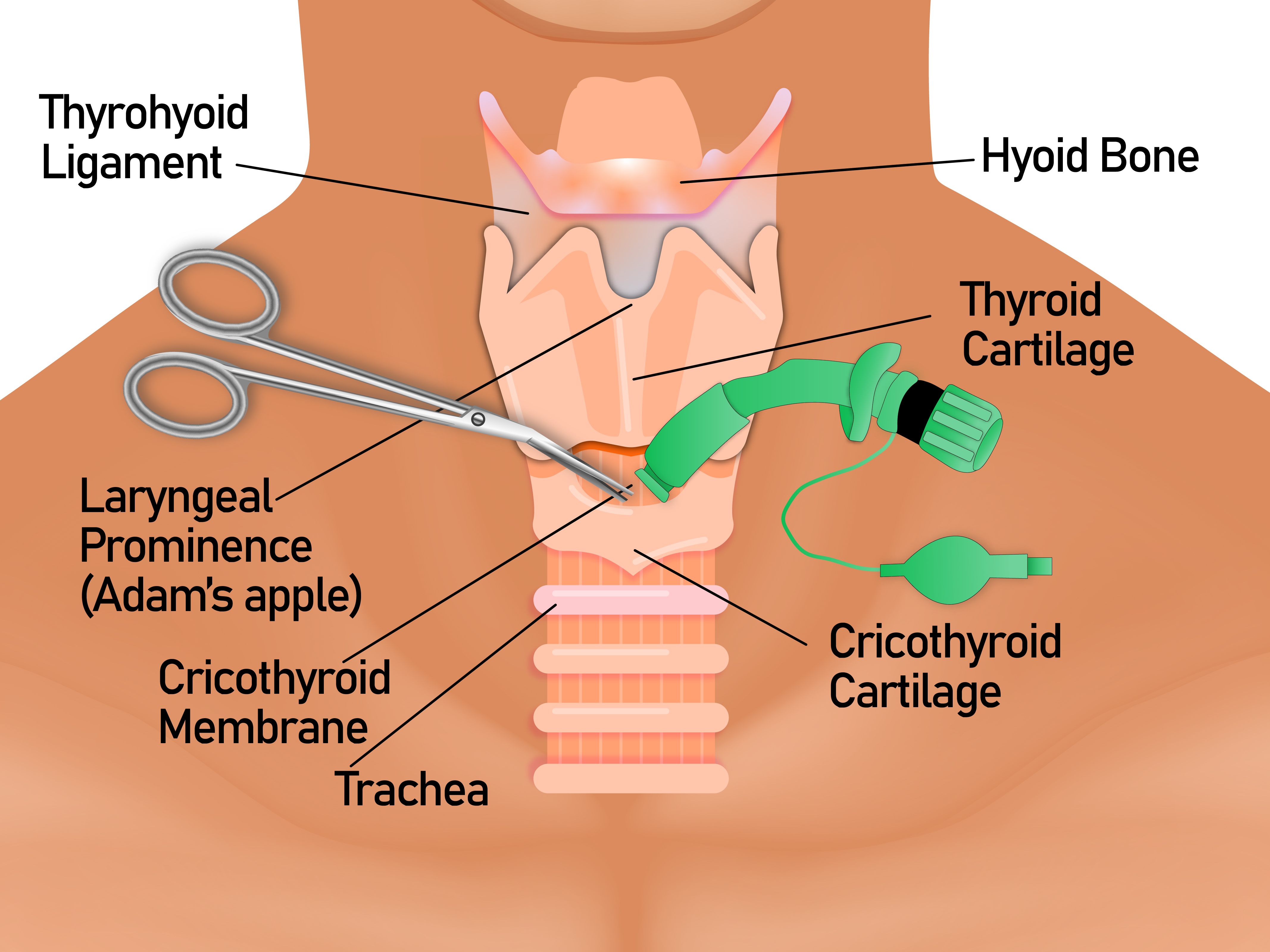
Cricothyrotomy is an emergency surgical airway established through the cricothyroid membrane between the thyroid and cricoid cartilages. It's the definitive rescue airway when all non-surgical options have failed.
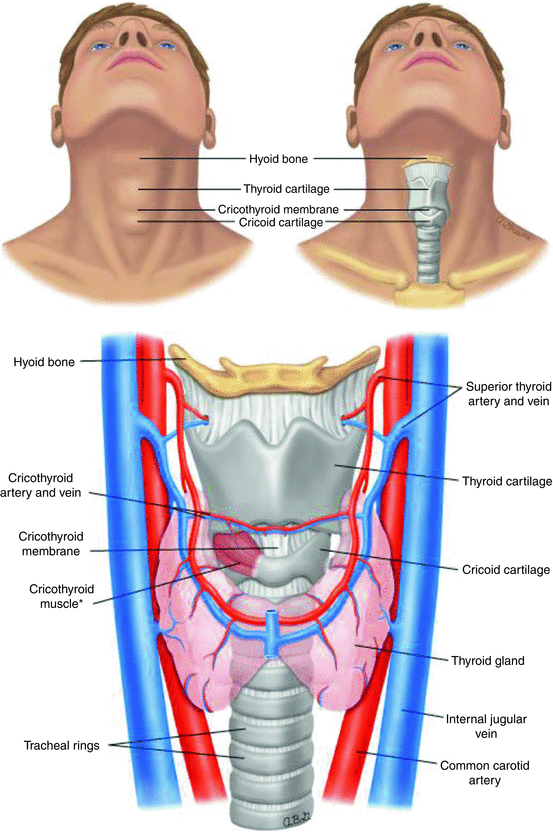
Understanding surface anatomy is critical for safe and rapid cricothyrotomy.
Have a dedicated cricothyrotomy kit or standardized "scalpel–bougie–tube" setup ready wherever advanced airway management occurs.
The scalpel-bougie-tube technique is widely taught and uses commonly available equipment.
Needle cricothyrotomy is primarily a temporizing measure, more commonly used in smaller children. It provides oxygenation but not effective CO₂ elimination.