Medical Disclaimer
- For Educational Purposes Only: This content is intended for educational reference and should not be used for clinical decision-making.
- Not a Substitute for Professional Judgment: Always consult your local protocols, institutional guidelines, and supervising physicians.
- Verify Before Acting: Users are responsible for verifying information through authoritative sources before any clinical application.
AI Assistance Notice
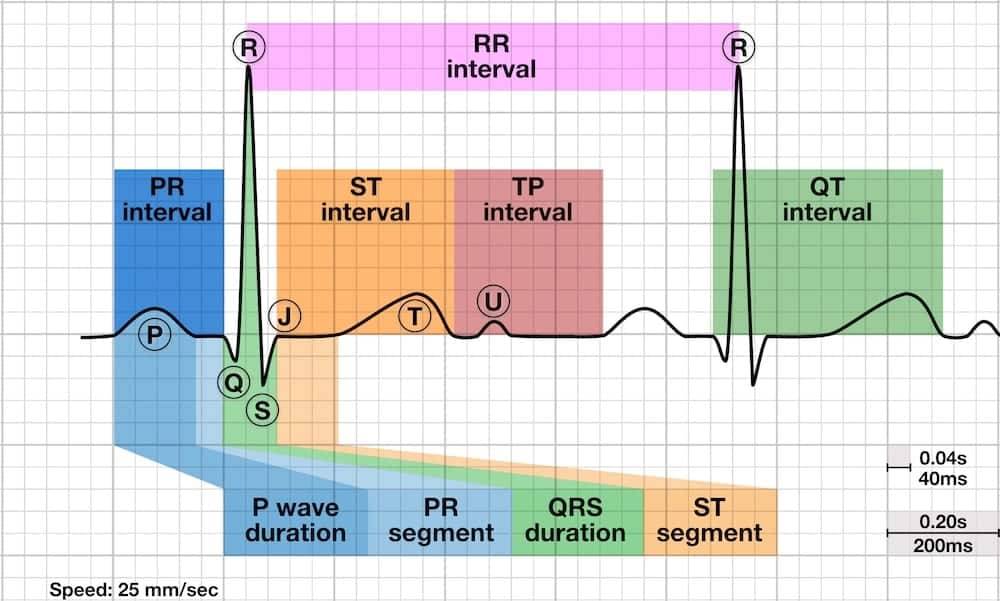
The S wave is any downward (negative) deflection that follows an R wave in the QRS complex. It represents the later phase of ventricular depolarization, particularly the activation of the posterobasal ventricular walls.
| Parameter | Normal Values | Clinical Significance |
|---|---|---|
| Definition | Any negative deflection after an R wave | Part of QRS complex, represents late ventricular depolarization |
| Normal V1 depth | Variable, typically 5-20 mm | Deeper S waves in V1-V2 are normal as left ventricle depolarizes away from right precordial leads |
| Normal V5-V6 depth | Usually small or absent | Minimal S wave in lateral leads as depolarization is toward these electrodes |
| Transition zone | V3-V4 (R/S ratio = 1) | Where R wave height equals S wave depth; shift indicates axis deviation or hypertrophy |
| Deep S waves | S in V1-V2 >15mm or S in V5-V6 >7mm | May indicate ventricular hypertrophy or conduction abnormality |
Electrical Genesis
The S wave represents the final phase of ventricular depolarization:
- Vector III (Terminal Depolarization): Activation of posterobasal right and left ventricular free walls, including the basal right septal mass and crista supraventricularis
- Direction: Resultant electrical force is directed rightward and posteriorly, away from left precordial leads
- Magnitude: Small compared to earlier vectors, reflecting the smaller muscle mass of the basal regions
- Left Ventricular Mass Effect: The larger the left ventricular muscle, the deeper the S wave in V1 and V2
Normal S Wave Distribution
S wave depth varies systematically across ECG leads:
- Right Precordial Leads (V1-V2): Deep S waves are normal - depolarization travels away from these electrodes toward the larger left ventricle
- Mid-Precordial Leads (V3-V4): Transition zone where R wave height equals S wave depth (R/S ratio = 1)
- Left Precordial Leads (V5-V6): S waves are minimal or absent - depolarization travels toward these electrodes
- Limb Leads: S wave depth varies with cardiac axis; deep S in lead I suggests right axis deviation
S Wave Nomenclature
- Uppercase "S": Denotes a large (≥5mm) negative deflection after R wave
- Lowercase "s": Denotes a small (<5mm) negative deflection after R wave
- Terminal s: Small S wave at end of QRS, seen in some lateral leads with counterclockwise rotation
- Slurred S: Widened, notched S wave seen in bundle branch blocks
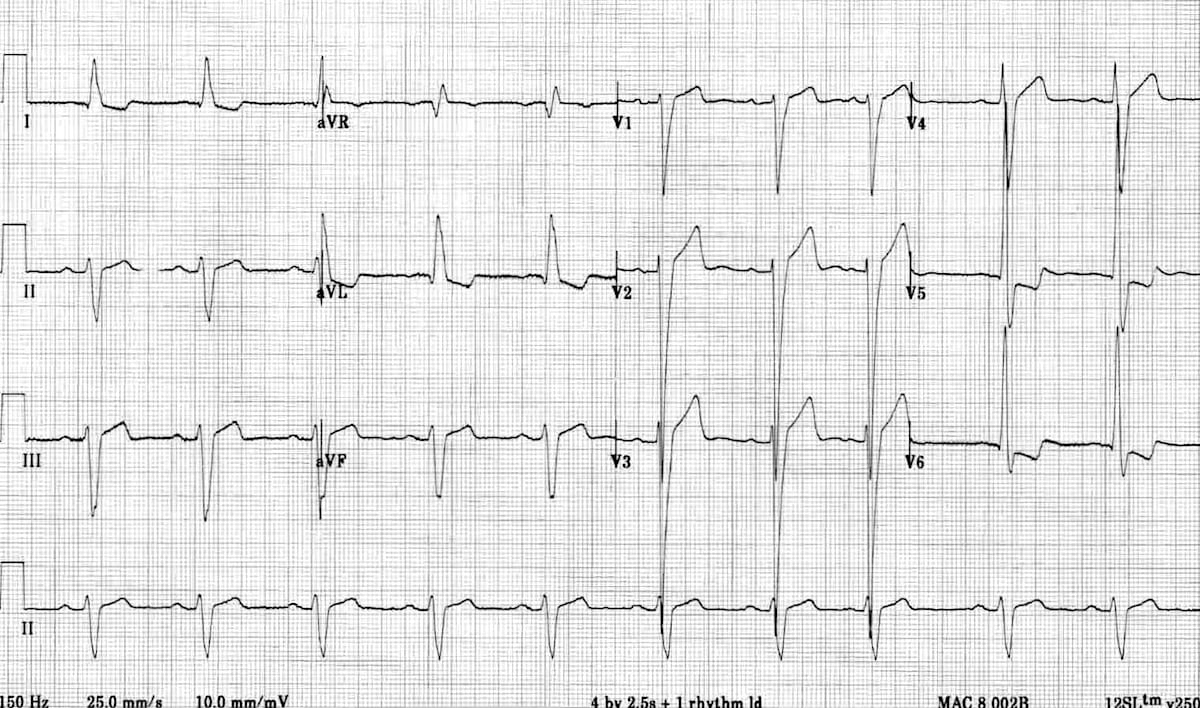
Left ventricular hypertrophy causes increased QRS voltages, particularly deep S waves in right precordial leads and tall R waves in left precordial leads.
Pathophysiology
- Increased Muscle Mass: Thickened LV wall generates larger electrical forces during depolarization
- Prolonged Depolarization: More muscle requires longer time to depolarize, widening QRS slightly
- Vector Magnitude: Larger leftward and posterior forces create deeper S waves in right-facing leads (V1-V3)
- Repolarization Changes: Secondary ST-T changes (strain pattern) due to altered repolarization sequence
Voltage Criteria for LVH
| Criterion | Threshold | Specificity |
|---|---|---|
| Sokolow-Lyon | S in V1 + R in V5 or V6 > 35 mm | ~90% |
| Cornell (Men) | R in aVL + S in V3 ≥ 24 mm | ~90% |
| Cornell (Women) | R in aVL + S in V3 ≥ 18 mm | ~90% |
| Age <30 years | S in V1 + R in V5/V6 > 40 mm | Higher threshold for younger patients |

LV Strain Pattern
Accompanies voltage criteria in severe LVH:
- ST Depression: Downsloping ST segment in lateral leads (I, aVL, V5-V6)
- T Wave Inversion: Asymmetric T wave inversion in lateral leads
- Mechanism: Delayed repolarization from endocardium to epicardium due to increased wall thickness
- Prognosis: Strain pattern associated with worse outcomes - indicates significant hypertrophy
Causes of LVH
- Hypertension: Most common cause - chronic pressure overload
- Aortic Stenosis: Severe pressure overload from fixed obstruction
- Aortic Regurgitation: Volume overload with combined pressure load
- Hypertrophic Cardiomyopathy: Primary genetic disorder with massive hypertrophy
- Athletic Heart: Physiologic hypertrophy in endurance athletes (no strain pattern)
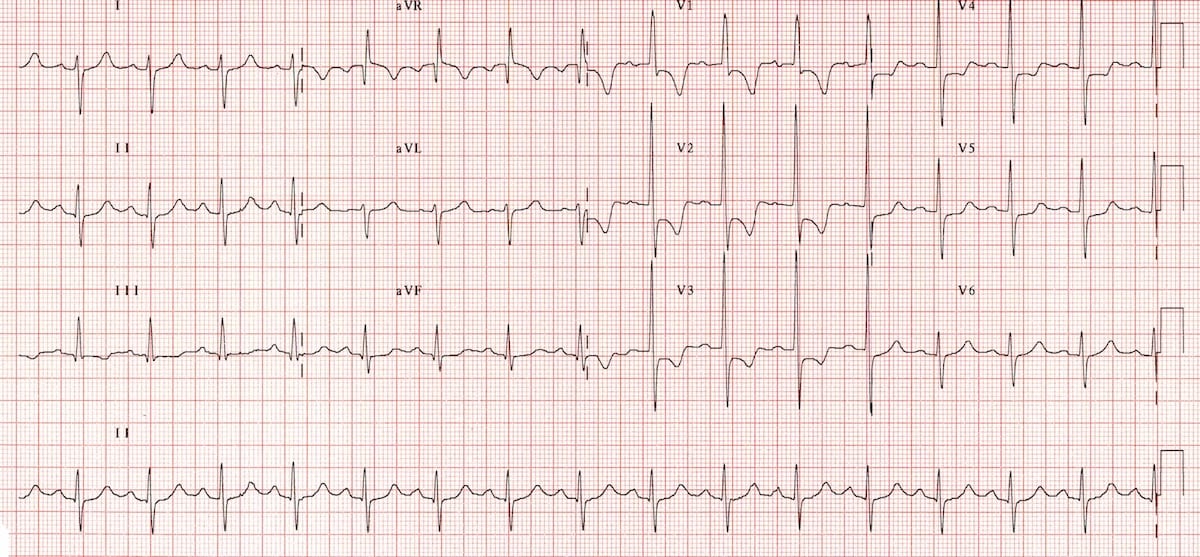
Right ventricular hypertrophy causes deep S waves in LEFT precordial leads (V5-V6), opposite to the pattern seen in LVH.
Diagnostic Criteria for RVH
RVH requires at least 2 of the following:
- Right Axis Deviation: ≥ +110° (required for diagnosis)
- Dominant R in V1: R wave ≥ 7 mm or R/S ratio > 1 in V1
- Deep S in V5 or V6: S wave ≥ 7 mm or R/S ratio < 1 in V5-V6
- QRS Duration: < 120 ms (changes not due to RBBB)
Supporting Criteria
- Right Atrial Enlargement: P pulmonale (peaked P > 2.5 mm in II)
- RV Strain Pattern: ST depression and T wave inversion in V1-V4, II, III, aVF
- S1S2S3 Pattern: Dominant S waves in leads I, II, and III (extreme right axis)
- Deep S in Lateral Leads: Deep S waves in I, aVL, V5-V6
Pathophysiology
- RV Dominance: Hypertrophied RV creates forces that oppose normal leftward vectors
- Axis Shift: Electrical axis shifts rightward as RV forces increase
- Lateral S Waves: Deep S in V5-V6 as depolarization moves away from lateral leads toward hypertrophied RV
- Strain: RV strain pattern indicates severe hypertrophy with pressure overload
Common Causes
- Pulmonary Hypertension: Most common cause in adults
- Chronic Lung Disease: Cor pulmonale from COPD, pulmonary fibrosis
- Pulmonary Embolism: Acute or chronic thromboembolic disease
- Mitral Stenosis: Increased RV pressure from left atrial hypertension
- Congenital Heart Disease: Tetralogy of Fallot, pulmonary stenosis, ASD
- ARVC: Arrhythmogenic right ventricular cardiomyopathy
Right Bundle Branch Block (RBBB)
RBBB creates characteristic wide, slurred S waves in lateral leads:
- Wide Slurred S in I, V5, V6: Terminal S wave >40 ms in duration
- Mechanism: Delayed right ventricular depolarization creates late rightward forces
- RSR' in V1-V2: Characteristic "M" pattern with terminal R wave in right precordial leads
- QRS Duration: ≥ 120 ms for complete RBBB, 100-119 ms for incomplete RBBB
- S Wave Duration > R Wave: In lateral leads, the S wave amplitude may exceed the preceding R wave
Left Bundle Branch Block (LBBB)
LBBB affects S wave morphology differently:
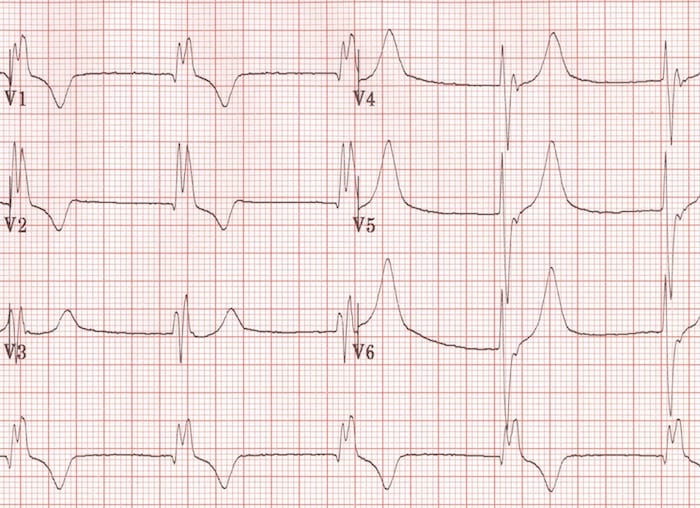
- Deep S or QS in V1-V2: Absent R wave with deep QS complex in right precordial leads
- Absent Septal Q Waves: No small q waves in lateral leads (I, aVL, V5-V6)
- Mechanism: Septal depolarization occurs right-to-left (reversed), eliminating normal septal forces
- Broad Monophasic R in V5-V6: No S wave in lateral leads - smooth R wave without notching
- QRS Duration: ≥ 120 ms with broad, notched morphology
Clinical Significance
- RBBB: Often benign in young adults; may indicate RV strain (PE, pulmonary HTN) or structural disease in older patients
- LBBB: Almost always indicates underlying cardiac disease (CAD, cardiomyopathy, HTN, aortic valve disease)
- New LBBB + Chest Pain: Consider STEMI equivalent - urgent cardiology consultation
- Bifascicular Block: RBBB + left axis deviation suggests two-level conduction disease
The S1S2S3 pattern refers to dominant S waves in limb leads I, II, and III, indicating extreme right axis deviation.
Definition and Recognition
- Lead I: S wave deeper than R wave is tall (R/S < 1)
- Lead II: S wave deeper than R wave is tall
- Lead III: S wave deeper than R wave is tall
- Axis: Typically > +120° to +180° (far right axis)
Clinical Associations
- Right Ventricular Hypertrophy: Most common cause - chronic RV pressure overload
- Acute Pulmonary Embolism: Part of classic PE triad (S1Q3T3 pattern)
- Chronic Pulmonary Disease: Cor pulmonale with RV strain
- Normal Variant: Rarely seen in thin, tall individuals with vertical heart orientation
- Left Posterior Fascicular Block: Can produce similar pattern with right axis
Pulmonary Embolism (S1Q3T3)
Classic ECG pattern of acute PE (present in only ~20% of cases):
- S wave in Lead I: Deep S wave indicating right axis shift
- Q wave in Lead III: Q wave with T wave inversion in III
- T inversion in Lead III: Right ventricular strain
- Additional Findings: Sinus tachycardia, right axis deviation, RBBB, T wave inversion in V1-V4
Differential Diagnosis of S1S2S3
| Condition | Key Distinguishing Features |
|---|---|
| Chronic RVH | Tall R in V1, deep S in V6, P pulmonale, gradual onset |
| Acute PE | Sudden onset, S1Q3T3, sinus tachycardia, T inversion V1-V4 |
| COPD | Low voltage, P pulmonale, signs of hyperinflation |
| LPFB | Right axis >+120°, qR in III/aVF, rS in I/aVL |
The transition zone is where R wave height equals S wave depth (R/S ratio = 1), normally occurring at V3 or V4.
Early Transition (V2 or Earlier)
Transition zone shifts leftward (toward V1-V2):
- Posterior Myocardial Infarction: Loss of posterior forces creates early R wave dominance in V1-V2
- Right Ventricular Hypertrophy: Increased RV forces shift transition leftward
- WPW Syndrome Type A: Pre-excitation creates tall R in V1-V2
- Normal Variant: Especially in children and young adults
- Clockwise Rotation: Heart rotates so left ventricle faces more anteriorly
Delayed Transition (V5 or Later)
Transition zone shifts rightward (toward V5-V6):
- Left Ventricular Hypertrophy: Increased LV forces prolong S waves in right-to-mid precordial leads
- Anterior Myocardial Infarction: Loss of anterior forces delays R wave progression
- Left Bundle Branch Block: Altered depolarization sequence shifts transition
- Counterclockwise Rotation: Heart position shifts so left ventricle faces more leftward
- COPD: Hyperinflated lungs create vertical heart orientation
Persistent S Waves (No Transition)
S waves present across all precordial leads:
- Extreme Right Axis Deviation: S waves in all precordial and limb leads
- Severe RVH: Dominant right ventricular forces
- COPD with Cor Pulmonale: Vertical heart with RV enlargement
- Sokolow-Lyon is quick but imperfect: High specificity (~90%) but low sensitivity (<40%) for LVH - many patients with echo-confirmed LVH have normal voltage
- Age matters: S + R voltages normally higher in young adults (age <30: use >40mm cutoff); lower in elderly due to chest wall changes
- Body habitus affects voltages: Thin patients have higher voltages; obese patients have lower voltages - don't over-interpret in extremes
- Deep S in V2-V3 is normal: Don't be alarmed by 15-20mm S waves in V2 in healthy young adults - it's the left ventricle depolarizing away
- Slurred S waves are pathologic: Wide, notched S waves in lateral leads suggest RBBB; measure S wave duration - if >40ms, consider conduction delay
- S wave in aVR: Deep S in aVR is normal and expected; absence suggests lead reversal or dextrocardia
- Poor R progression mimics: Persistent S waves across precordium may be LVH, not anterior MI - check for tall R in V5-V6
- Athletic heart syndrome: Can meet voltage criteria for LVH but lacks strain pattern and has normal repolarization
- S1S2S3 in PE is rare: Only ~20% of PE cases show S1Q3T3 pattern; most common ECG finding in PE is sinus tachycardia
- New RBBB + deep S: In context of dyspnea, consider acute PE causing acute RV strain and new conduction delay
Systematic S Wave Assessment
- Measure S Wave Depth in V1:
- Normal: 5-20 mm
- Deep (>20mm): Consider LVH if tall R in V5-V6
- Absent: Consider RVH, posterior MI, or WPW Type A
- Measure S Wave Depth in V5-V6:
- Normal: Minimal or absent
- Deep (>7mm): Consider RVH with R/S <1
- Persistent large S: Check for LVH or delayed transition
- Calculate Sokolow-Lyon:
- Add S in V1 + tallest R in V5 or V6
- >35mm (>40mm if age <30): Consider LVH
- Must confirm with non-voltage criteria
- Identify Transition Zone:
- Where R = S (R/S ratio = 1)
- Normal: V3 or V4
- Early (V2): RVH, posterior MI, WPW
- Late (V5-V6): LVH, anterior MI, LBBB
- Assess S Wave Morphology:
- Narrow: Normal depolarization
- Wide/slurred: Bundle branch block
- Measure duration: >40ms suggests conduction delay
Common Interpretation Pitfalls
- Mistake #1: Diagnosing LVH on voltage alone - MUST have supporting criteria (LAE, strain, increased RWPT)
- Mistake #2: Missing lead placement errors - check if S waves are unexpectedly absent or present where they shouldn't be
- Mistake #3: Over-calling LVH in young, thin patients - high voltages are normal in this population
- Mistake #4: Confusing poor R progression with persistent S waves - they're different patterns
- Mistake #5: Forgetting age-adjusted criteria - older patients have lower voltages, younger have higher
When to Suspect Technical Error
- S waves in unexpected leads: If S dominant in leads where R should be (e.g., all lateral leads), consider lead reversal
- Absent S in V1-V2: Unless RVH or posterior MI, should have some S wave - check lead placement
- Bizarre S wave morphology: Irregular, jagged S waves may indicate artifact or muscle tremor
- Asymmetric S waves: If one precordial lead has S wave vastly different from adjacent leads, verify placement
- Farkas, Josh MD. (2015). Table of Contents - EMCrit Project. EMCrit Project. https://emcrit.org/ibcc/toc/
- Khan, M. G. (2007). Rapid ECG Interpretation. Humana.
- Sigg, D. C., Iaizzo, P. A., Xiao, Y.-F., Bin He, & Springerlink (Online Service). (2010). Cardiac Electrophysiology Methods and Models. Springer Us.
- Wang, K. (2012). Atlas of Electrocardiography. JP Medical Ltd.
- ECG Library • LITFL • ECG Library Basics. (2018). Life in the Fast Lane • LITFL • Medical Blog. https://litfl.com/ecg-library/