Medical Disclaimer
- For Educational Purposes Only: This content is intended for educational reference and should not be used for clinical decision-making.
- Not a Substitute for Professional Judgment: Always consult your local protocols, institutional guidelines, and supervising physicians.
- Verify Before Acting: Users are responsible for verifying information through authoritative sources before any clinical application.
AI Assistance Notice
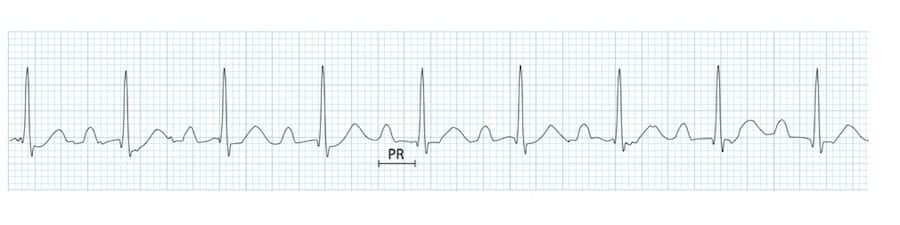
The PR interval is the time from the onset of the P wave to the start of the QRS complex. It represents the total time for an impulse to travel from the SA node through the atria, AV node, and His-Purkinje system to the ventricles.
The PR interval reflects AV nodal conduction time and is one of the most important markers of cardiac conduction system function. Understanding PR interval abnormalities is essential for:
- Diagnosing AV blocks: First, second, and third-degree heart block
- Identifying preexcitation: WPW syndrome, LGL syndrome, enhanced AV conduction
- Assessing drug effects: Beta-blockers, calcium channel blockers, digoxin
- Recognizing junctional rhythms: Short PR with retrograde P waves
- Risk stratification: Prolonged PR associated with heart failure, syncope risk
Physiologic Components of the PR Interval
The PR interval consists of three main components:
- Atrial conduction time (~30-40 ms): Impulse spread through atrial myocardium
- AV nodal delay (~90-100 ms): Physiologic delay in AV node (majority of PR interval)
- His-Purkinje conduction (~30-55 ms): Rapid conduction through specialized conduction system
Source: LITFL - ECG waves, segments and intervals
URL: https://litfl.com/wp-content/uploads/2018/10/ECG-waves-segments-and-intervals-LITFL-ECG-library-3.jpg
Save as:
/education/medical/Cardiac/pr-interval/ecg-waves-segments-intervals.jpg
Normal Range and Measurement
- Duration: 0.12 to 0.20 seconds (120-200 milliseconds)
- ECG paper: 3 to 5 small squares at standard 25 mm/sec speed
- Measurement start: Beginning of P wave (first deflection from baseline)
- Measurement end: Beginning of QRS complex (first deflection of Q, R, or S wave)
- Lead selection: Measure in lead with clearest P wave and QRS onset (usually lead II or V1)
Age-Related Variations
| Age Group | Normal PR Range | Notes |
|---|---|---|
| Newborn | 0.08-0.16 sec | Shorter PR due to smaller cardiac size |
| Infant (1-12 mo) | 0.08-0.15 sec | Gradually lengthens with growth |
| Child (1-10 yr) | 0.10-0.18 sec | Approaches adult values |
| Adolescent/Adult | 0.12-0.20 sec | Standard adult range |
| Elderly | 0.12-0.22 sec | Slight prolongation common with aging |
Heart Rate Effects
The PR interval is inversely related to heart rate:
- Tachycardia: PR shortens (AV node conducts faster with increased sympathetic tone)
- Bradycardia: PR lengthens (increased vagal tone slows AV conduction)
- Clinical pearl: A PR of 0.18-0.20 sec at rest that shortens to 0.12-0.14 sec with exercise is normal
- Warning: PR that lengthens with exercise suggests AV nodal disease
Definition & Criteria
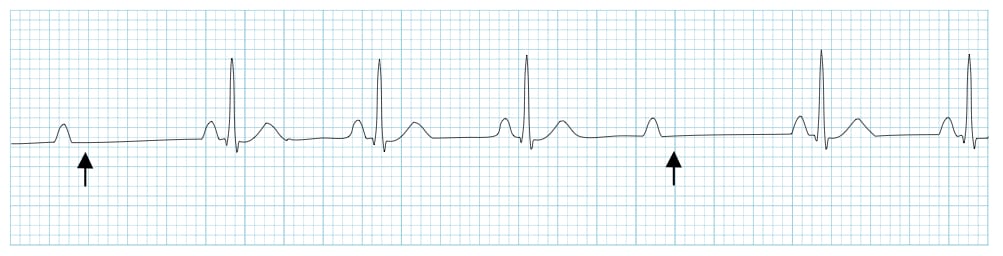
First-degree AV block is defined as a prolonged PR interval >0.20 seconds (>5 small boxes) with 1:1 AV conduction - every P wave is followed by a QRS complex.
 0.20 seconds"
style="max-width: 700px; max-height: 400px; width: 100%; height: auto; object-fit: contain;">
0.20 seconds"
style="max-width: 700px; max-height: 400px; width: 100%; height: auto; object-fit: contain;">
Mechanism
- Site of delay: Most commonly in the AV node (intranodal), but can occur in the atrium, bundle of His, or bundle branches
- Physiology: Slowed conduction through the AV junction; all impulses eventually conduct
- Functional impact: Usually benign; rarely causes symptoms unless PR is extremely prolonged (>0.30 sec)
Causes of Prolonged PR Interval
| Category | Specific Causes |
|---|---|
| Medications | Beta-blockers, calcium channel blockers (diltiazem, verapamil), digoxin, amiodarone, class IA/IC antiarrhythmics |
| Increased vagal tone | Athletes, sleep, vagal maneuvers |
| Degenerative disease | Lenegre disease, Lev disease (age-related fibrosis) |
| Ischemia/Infarction | Inferior MI (RCA supplying AV node), septal MI |
| Inflammatory | Myocarditis, Lyme disease, rheumatic fever, endocarditis |
| Infiltrative | Sarcoidosis, amyloidosis, hemochromatosis |
| Metabolic | Hyperkalemia, hypothyroidism |
| Congenital | ASD, Ebstein anomaly, maternal SLE (neonatal lupus) |
Clinical Significance
- Benign in most cases: Typically asymptomatic and requires no treatment
- Medication review: Consider dose reduction if on AV nodal blocking agents
- Risk of progression: Low risk in asymptomatic patients; higher risk with structural heart disease or symptoms
- "Pacemaker syndrome": Very long PR intervals (>0.30 sec) can cause atrial contraction against closed AV valves, mimicking pacemaker syndrome with fatigue, dyspnea, or presyncope
Second-degree AV block occurs when some (but not all) atrial impulses fail to conduct to the ventricles. There are two main types with distinct mechanisms, locations, and clinical implications.
Mobitz Type I (Wenckebach)
- Pattern: Progressive lengthening of the PR interval until a P wave fails to conduct (dropped QRS)
- Grouping: QRS complexes occur in groups (e.g., 3:2, 4:3, 5:4 conduction ratios)
- PR interval behavior: Longest PR immediately before the dropped beat; shortest PR immediately after the dropped beat
- RR interval behavior: Progressive shortening of RR intervals before the pause; pause is less than twice the shortest RR
- Site of block: AV node (above the bundle of His)

Clinical Context for Mobitz I
- Often benign: Common in athletes, during sleep, or with increased vagal tone
- Reversible causes: Medications (beta-blockers, CCBs, digoxin), inferior MI (usually transient)
- Prognosis: Generally good; rarely progresses to complete heart block
- Treatment: Usually observation; treat underlying cause; rarely requires pacing unless symptomatic
Mobitz Type II
- Pattern: Sudden, unexpected dropped QRS without preceding PR prolongation
- PR interval behavior: Constant PR interval for conducted beats
- QRS morphology: Often wide (≥0.12 sec) due to infranodal location of block
- Site of block: Bundle of His or bundle branches (infranodal)
- Conduction ratio: Can be fixed (e.g., 2:1, 3:1) or variable
Clinical Context for Mobitz II
- Pathologic: Always abnormal; indicates significant conduction system disease
- High risk: Can progress unpredictably to complete heart block
- Associated with: Anterior MI, degenerative conduction disease, structural heart disease
- Treatment: Pacemaker typically indicated, especially if symptomatic or wide QRS
2:1 AV Block (Special Case)
When every other P wave conducts (2:1 pattern), you cannot determine if it's Mobitz I or II because there's no opportunity to observe PR interval behavior. Clues to differentiate:
- Mobitz I more likely if: Narrow QRS, inferior MI, reversible cause present
- Mobitz II more likely if: Wide QRS (bundle branch block pattern), anterior MI, no reversible cause
- When in doubt: Treat as potentially Mobitz II (higher risk); consider pacemaker evaluation
A PR interval <0.12 seconds indicates either rapid AV conduction or bypass of the normal AV node delay. This can be normal variant or pathologic preexcitation.
Causes of Short PR Interval
| Condition | PR Interval | QRS Morphology | Clinical Significance |
|---|---|---|---|
| Wolff-Parkinson-White (WPW) | <0.12 sec | Wide with delta wave (slurred upstroke) | Accessory pathway; risk of SVT, AFib with RVR |
| Lown-Ganong-Levine (LGL) | <0.12 sec | Normal (narrow, no delta wave) | Enhanced AV nodal conduction; controversial entity |
| Junctional/Low atrial rhythm | <0.12 sec or absent | Normal (narrow) | Ectopic pacemaker near AV node |
| Normal variant (athletic/young) | 0.10-0.11 sec | Normal | Benign; no delta wave |
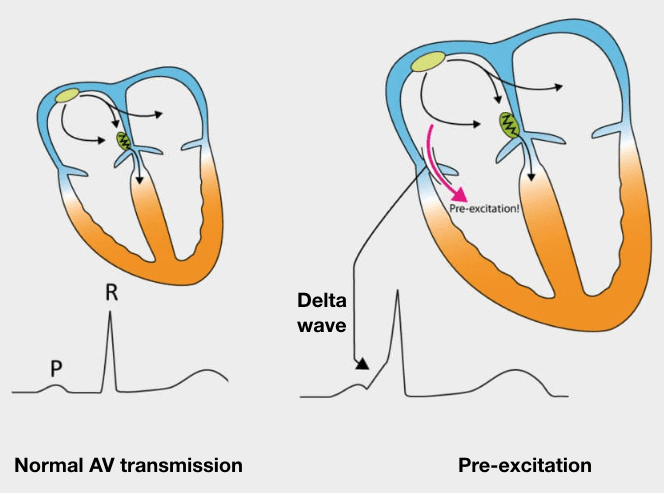
Wolff-Parkinson-White (WPW) Syndrome
- Mechanism: Accessory pathway (bundle of Kent) bypasses AV node, causing early ventricular activation
- ECG features:
- Short PR interval (<0.12 sec)
- Wide QRS (>0.12 sec) due to fusion of normal and preexcited conduction
- Delta wave: slurred, slow upstroke at beginning of QRS
- Secondary ST-T changes opposite to QRS direction
- Arrhythmia risks:
- AVRT (AV reentrant tachycardia) - most common
- Atrial fibrillation with rapid ventricular response via accessory pathway (can degenerate to VFib - medical emergency!)
Lown-Ganong-Levine (LGL) Syndrome
- Definition: Short PR interval (<0.12 sec) with normal QRS (no delta wave)
- Proposed mechanism: Enhanced AV nodal conduction or James fibers (bypass tract)
- Controversy: Many experts consider this a normal variant rather than true syndrome
- Arrhythmia risk: Debated; some patients develop SVT, but causal relationship unclear
Differentiating WPW from LGL
- WPW = short PR + wide QRS + delta wave (ventricular preexcitation via accessory pathway)
- LGL = short PR + normal QRS + no delta wave (rapid AV conduction, no ventricular preexcitation)
- Normal PR interval: 0.12-0.20 seconds (3-5 small boxes at standard speed)
- Measurement: Start of P wave to start of QRS complex
- Represents: Atrial depolarization + AV nodal delay + His-Purkinje conduction
- Short PR: <0.12 seconds (preexcitation, enhanced AV conduction, junctional rhythm)
- Prolonged PR: >0.20 seconds (first-degree AV block)
- Variable PR: Suggests higher-degree AV block (Mobitz I, Mobitz II, or third-degree)
- Key pearl: PR interval changes with heart rate - shortens with tachycardia, lengthens with bradycardia
- Farkas, Josh MD. (2015). Table of Contents - EMCrit Project. EMCrit Project. https://emcrit.org/ibcc/toc/
- Khan, M. G. (2007). Rapid ECG Interpretation. Humana.
- Sigg, D. C., Iaizzo, P. A., Xiao, Y.-F., Bin He, & Springerlink (Online Service). (2010). Cardiac Electrophysiology Methods and Models. Springer Us.
- Wang, K. (2012). Atlas of Electrocardiography. JP Medical Ltd.
- ECG Library • LITFL • ECG Library Basics. (2018). Life in the Fast Lane • LITFL • Medical Blog. https://litfl.com/ecg-library/